What the quality of work means for our health
What the quality of work means for our health
4 February 2020
About 13 mins to read
Key points
- Work is a key influence on health. Work matters for health directly, as well as underpinning other factors that influence health such as income or social networks.
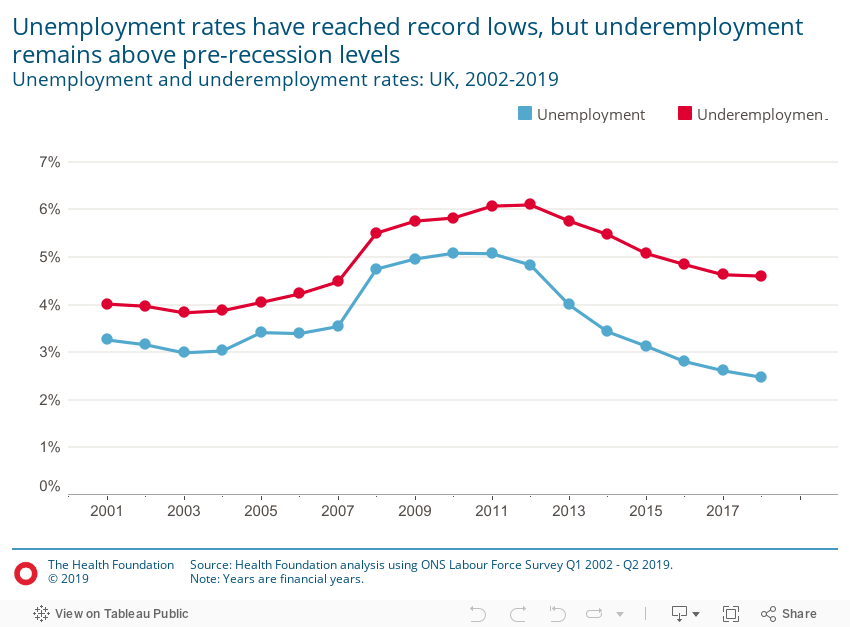
- The UK’s high employment level means that attention should shift from the association between unemployment and health, to the impact that the quality of work has on health.
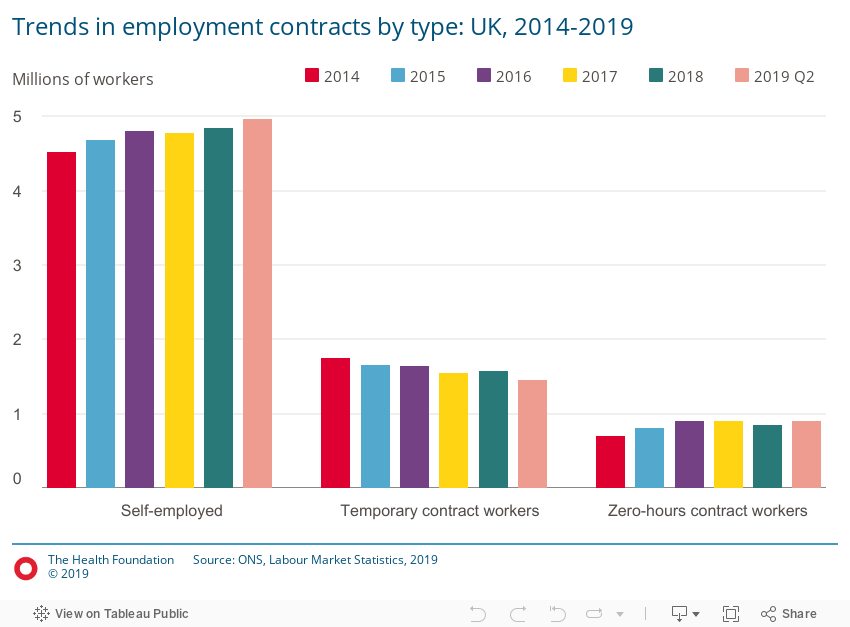
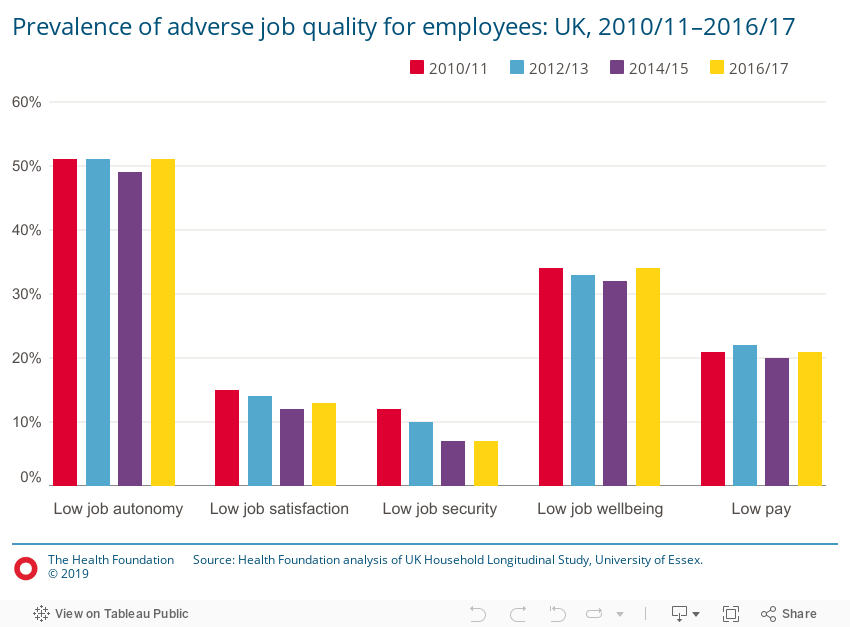
- Job insecurity (for example, zero-hours contracts) receives a lot of policy and media attention. However, this is only one aspect of low-quality work. A job can be secure and still be considered low quality.
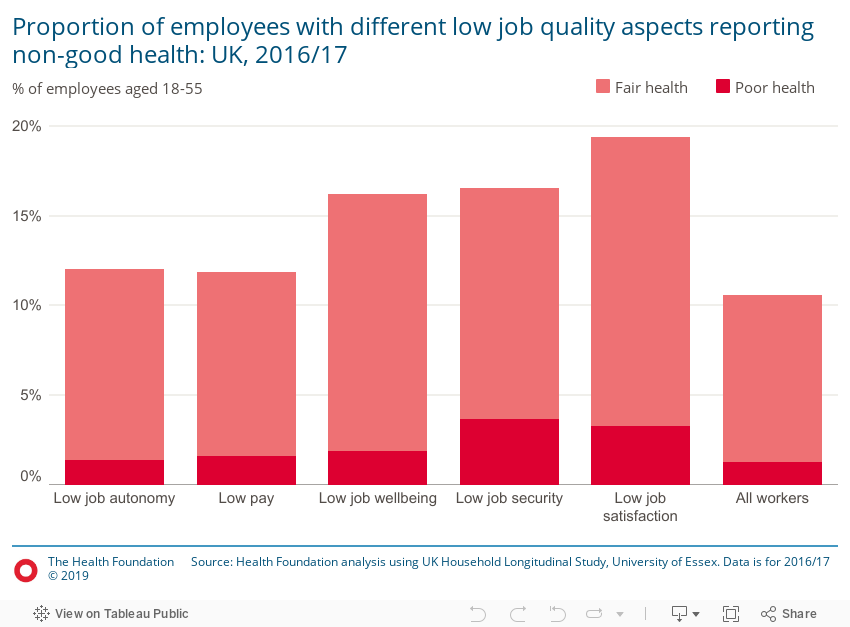
- This piece presents a broader measure of low-quality work, which incorporates subjective indicators of low levels of autonomy, negative emotions associated with a job, security and satisfaction, and other aspects of job quality from survey data, as well as low pay. The more of these factors that people experience in their work, the more likely they are to have worse health.
- Using the broader measure, over one-third (36%) of employees report being in low-quality work. Of these, 15% report experiencing poorer health – which is twice as high than for those with no negative job aspects, at 7%.
- Half of those in low-quality work in 2010/11 were still in low-quality work in 2016/17. Spending longer in low-quality work is associated with worse health outcomes. Low-quality work can trigger stress, and the damage stress does to the body builds over time.
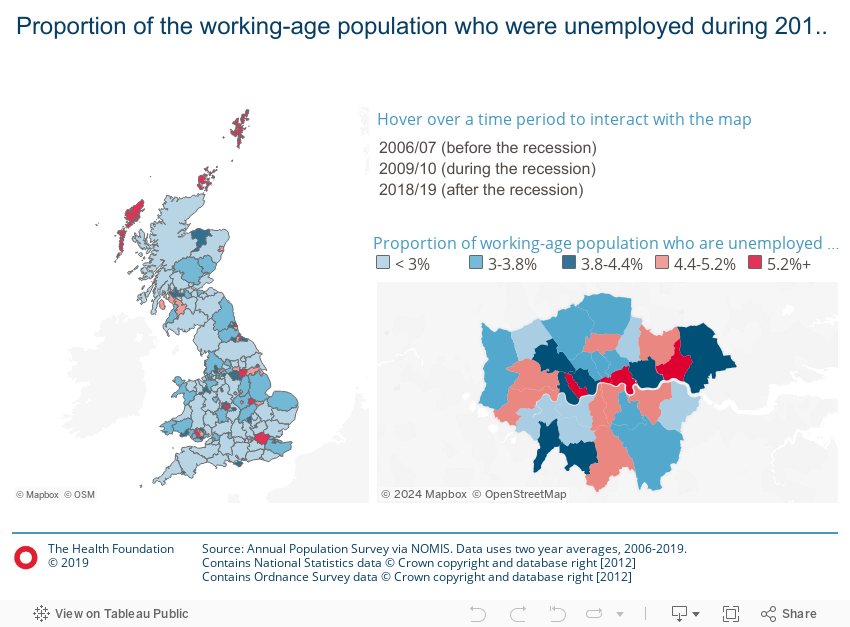
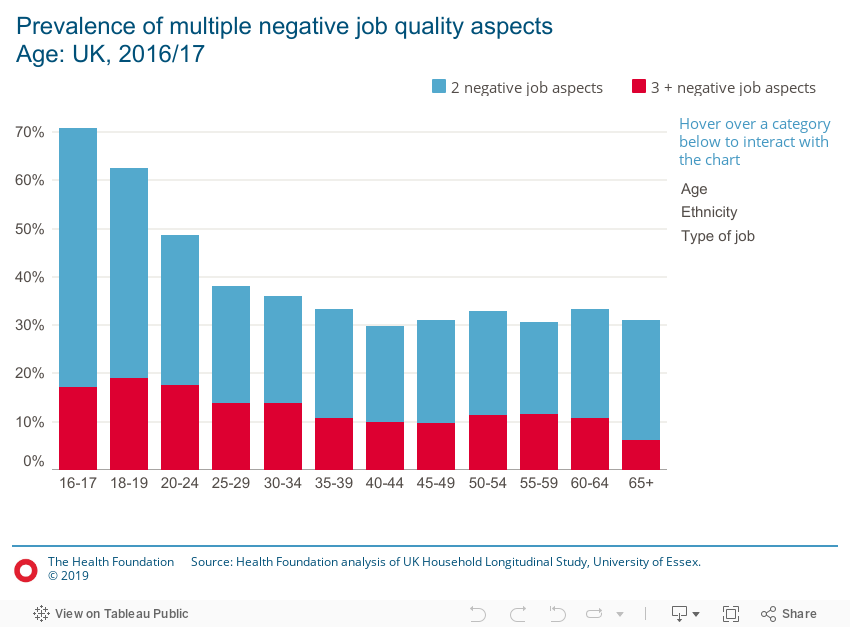
- Low-quality work is unequally distributed across society, both in terms of geography and demography, reflecting broader inequalities. Certain groups are more likely to be in low-quality work including younger adults, people in more routine occupations, and members of black and minority ethnic groups.
- High employment levels have not resulted in better job quality. There has been little change in the extent to which people report low job quality since 2010/11. With the UK’s employment law set for review as it leaves the EU, action is needed to improve job quality. Beyond regulatory fixes, employers should give greater consideration to job security, job design, management practices and the working environment to boost job quality.
For our latest analysis of work and health, visit our What drives health inequalities? evidence hub.

Explore our full analysis
Discover
Evidence hub: What drives health inequalities?
Discover
Data and insight highlighting how the circumstances in which we live shape our opportunities for...

What the quality of work means for our health
Work with us
We look for talented and passionate individuals as everyone at the Health Foundation has an important role to play.
View current vacanciesThe Q community
Q is an initiative connecting people with improvement expertise across the UK.
Find out more

{kind=link}